Caso ClÃnico
Intracoronary lithotripsy for stent underexpansion resolution: utility of enhanced stent visualization or StentVizâ„¢
Juan Mieres, Carlos Fernández-Pererira, Diego Ascarrunz, MatÃas RodrÃguez-Granillo, Alfredo E RodrÃguez
Revista Argentina de Cardioangiología Intervencionista 2022;(2): 0077-0080 | Doi: 10.30567/RACI/20222/0077-0080
Percutaneous coronary intervention is always supported by elements of innovative technologyto create solutions to everyday problems that are complex like the management of severely calcified plaques, and a complication that is sometimes unexpected, which is stent underexpansion that can be truly challenging. We present three cases of stent underexpansion throughout different time periods, the first one presented in an acute form, and was solved within the first 24 hours. The second case was chronic stent underexpansion of several-month evolution that worsened due to the presence of acute coronary syndrome and that was solved in the same hospitalization. The last case was extremely challenging and involved the left main coronary artery that presented a slight stent underexpansion that, within a few months, became symptomatic and was successfully solved. All these cases were solved using intracoronary lithotripsy, a novel device that through ultrasound probes transmitted by a rapid exchange catheter breaks down coronary calcium. These were tested in de novo calcified plaques. We present patients who already had a previous stent and were guided by the stent enhancement technique, General Electric angiography systemStentViz™.It uses an algorithm to visualize the stent struts and allow detailed monitoring to achieve the proper stent expansion, which is associated with fewer cardiovascular events at follow-up.
Palabras clave: underexpansion of the stent, IVL, intracoronary lithotripsy, StentVizâ„¢, ESV, enhanced stent visualization.
La intervención percutánea siempre está apoyada en elementos de tecnología innovadora tratando de crear soluciones a problemas cotidianos que son complejos como el tratamiento de placas severamente calcificadas y una complicación a veces inesperada que es la subexpansión del stent, que puede ser un gran desafío. Presentamos tres casos de subexpansión en diferentes períodos de tiempo, el primero en forma aguda que pudo resolverse dentro de las primeras 24 horas, el segundo una subexpansión crónica de varios meses que se reagudizó por un síndrome coronario agudo y que se resolvió en la misma internación, y el tercero, muy desafiante, del tronco de coronaria izquierda que presentó una subexpansión leve que en pocos meses se volvió sintomática y fue resuelta exitosamente. Todos estos casos fueron resueltos con litotricia intracoronaria, novel dispositivo que a través de sondas ecográficas transmitidas por un catéter de rápido intercambio permite fracturar el calcio, estos fueron probados en placas de novo, presentamos pacientes que ya tenían un stent previo y guiados por la técnica del realce de la visualización del stent en los angiógrafos General Electric, llamado StentViz™, técnica que a través de un algoritmo permite claramente la visualización de los struts del stent y posibilita un seguimiento detallado para alcanzar una correcta expansión, que está asociada a disminución de los eventos cardiovasculares en el seguimiento.
Keywords: subexpansión del stent, IVL, litotricia intracoronaria, StentViz™, RVS, realce de la visualización del stent.
Los autores declaran no poseer conflictos de intereses.
Fuente de información Colegio Argentino de Cardioangiólogos Intervencionistas. Para solicitudes de reimpresión a Revista Argentina de CardioangiologÃa intervencionista hacer click aquí.
Recibido 2022-03-27 | Aceptado 2022-04-29 | Publicado

Esta obra está bajo una Licencia Creative Commons Atribución-NoComercial-SinDerivar 4.0 Internacional.


Introduction
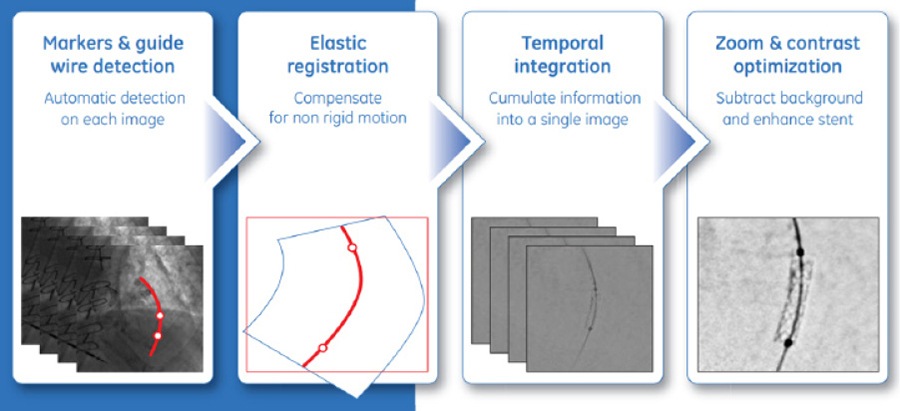
Complex angioplasties associated with heavily calcified plaques have always been challenging regarding percutaneous coronary interventions (PCI) in the routine clinical practice.1 There are 2 different devices available that we use daily in our cath labs to perform these PCIs: enhanced stent visualization (ESV), which is a technology provided by an angiographic system built by General Electric (GE, Boston, MA, United States), the so-called StentVizTM.2 It allows us to view the stent struts very rapidly (Figure 1). Secondly, all devices capable of treating these plaques, among them, rotational ablation,3 high and very-high pressure balloons that can reach up to 40 atmospheres,4,5 and finally intracoronary lithotripsy (ICL) (Shockwave Medical, Fremont, CA, United States)6 used to treat de novo plaques before stenting. However, there are times when the stent has already been implanted and stent underexpansion becomes a serious problem. We should mention that proper stent expansion is associated with fewer cardiovascular adverse events in the long term.7
We will be describing three different cases of stent underexpansion solved with StentVizTM-guided ICL.
Case presentation
Case #1
The patient was a 65-year-old man with type 2 diabetes and a severe lesion at the origin of the right coronary artery, another lesion in the proximal third, another in the middle third, and yet another moderate-to-severe lesion in the distal third. Also, the presence of severe calcification in the entire arterial trajectory was confirmed. PCI was started with predilatation of the ostial, proximal, and middle plaques using compliant and non-compliant balloons. Afterwards, a 3.0 mm x 23 mm stent (Waltz™, Microport, Shanghai, China) was implanted in the proximal third. The StentViz™ visualization tool confirmed the presence of severe stent underexpansion. Several attempts were made to expand the stent with different 3.0 mm, 3.5 mm, and 4.0 mm non-compliant balloons (FirefighterTM NC, Microport, Shanghai, China) for extended periods of time. Then, we rapidly thought of the different options available and decided to go with ICL. Then, we used one 2.5 mm x 15 mm Shockwave balloon at 4 atm and 6 atm (8 cycles, 10 pulses each) until completing 80 pulses. The entire procedure was closely monitored with the StentViz™ visualization tool. Balloon started expanding and the ICL was completed with a 3.0 mm non-compliant balloon (FirefighterTM NC, Microport, Shanghai, China) that was inflated at high atmospheres. We did not think it was necessary to implant another stent. In the lesion located at the middle third we performed a de novo ICL and a 3.0 mm x 23 mm stent (Waltz™, Microport, Shanghai, China) was implanted. A different 4.0 mm x 18 mm stent (Waltz™, Microport, Shanghai, China) was implanted into the ostium and the whole vessel showed a uniform appearance. The patient was discharged 48 hours later with clopidogrel, apixaban, and aspirin for 1 month plus colchicine for 3 months. The patient was on anticoagulation therapy due to AF (Figure 2).
The patient remained asymptomatic at 6-month follow-up.
Case #2
It is a 60-year-old man with a past medical history of heavy smoking and COVID-19-related ARDS 2 months before hospitalization with coronary artery disease and several previous angioplasties due to multivessel disease with known chronic stent underexpansion in the middle third of the left anterior descending coronary artery. While hospitalized the patient developed an acutely occluded left anterior descending coronary artery that was partially solved with the use of non-compliant balloons that were inflated at high atmospheres and extended inflations. A few months later, the patient is readmitted to our center with a STEMI at left anterior descending coronary artery level with an acute occlusion of the proximal-middle third. Occlusion is solved implanting a 3.0 mm x 18 mm stent (Firehawk, Microport, Shanghai, China) into the proximal-to-middle third resulting in flow restoration. An attempt is made to fully expand this plaque using several non-compliant balloons. However, due to the presence of persistent chronic exacerbated stent underexpansion, it is decided to complete the expansion with using ICL with a 3.0 mm x 12 mm balloon. A total of 80 pulses were delivered at 4 to 6 atmospheres at the location of stent underexpansion. Full expansion was achieved with a 3.5 mm x 20 mm non-compliant balloon (FirefighterTM NC, Microport, Shanghai, China) with excellent angiographic results. The patient was discharged on prasugrel and aspirin at 48 hours.
The patient remained asymptomatic at 4-month follow-up.
Case #3
It is a 63-year-old woman with a past medical history of smoking and dyslipidemia with previous coronary artery disease and multiple previous angioplasties since 2004, among them, 1 with acute myocardial infarction with cardiogenic shock that required the use of intra-aortic balloon pump. This year in January the last angioplasty was performed on the left main coronary artery due to mild stent underexpansion. Patient is discharged, but since her condition progresses into dyspnea, she is readmitted for reassessment at 2 months. The presence of severe restenosis due to stent underexpansion at left main coronary artery level is confirmed. Restenosis is thoroughly observed using the StentViz™ visualization tool (General Electric, Boston, MA, United States). Predilatation was decided using a 3.0 mm x 12 mm non-compliant balloon and inserting a Shockwave balloon-catheter system from left main coronary artery to left anterior descending coronary artery delivering 80 pulses. This results in the gradual expansion of the stent. Aferwards, complete expansion is attempted with a 4.0 mm x 15 mm non-compliant balloon (FirefighterTM NC, Microport, Shanghai, China). Then, an angioplasty is performed on the left circumflex artery proximal third and the procedure is completed with a kissing balloon with optimal results as confirmed on the StentViz™ visualization tool. The patient remains on prasugrel, aspirin, rosuvastatin, carvedilol, and fenofibric acid (Figure 3).
The patient remained asymptomatic at 3-month follow-up.
Discussion
We presented 3 complex cases of stent underexpansion, the first one an acute case, the second a chronically underexpanded stent, and the third one a subacute underexpansion. In the first case, despite predilatation and stent impaction the proper expansion was not achieved. In the second case, the underexpansion was exacerbated by STEMI. The third one was a case of stent underexpansion at left main coronary artery level. All these cases were directly guided by the ESV visualization tool manufactured by GE, StentVizTM.
There is no doubt that coronary artery calcification (CAC) has always been challenging because it prevents devices from navigating easily. Most important of all is that stent expansion cannot be fully achieved, which is associated with the occurrence of more cardiovascular events. CACs were solved with compliant balloons, non-compliant balloons, and very high-pressure balloons plus a series of different atherectomy techniques. However, these techniques are also associated with certain complications and even have the potential to be lethal.1,3-5.
The arrival of ICL has revolutionized the expansion of heavily calcified plaques easy and fast with a rapid exchange catheter giving the PCI an innovative tool. The first presentation of this device was made by Brinton et al. in TCT back in 2016 where the DISRUPT CAD trial was introduced for the first time. This multicenter study conducted in 5 countries included heavily calcified plaques treated primarily with OCT-guided ICL. Favorable results were seen in a significant number of patients.6,7 Afterwards, the results from the DISRUPT CAD II, DISRUPT CAD III, and DISRUPT CAD IV clinical trials were reported.8-10
In previous issues of our journal, we have already reported on 4 cases of primary ICL in heavily calcified plaques or that could not be dilated with non-compliant balloons as our first experience in our region11 with very good short-term results. Now we are reporting 3 cases of stent underexpansion treated with ICL and guided by the ESV visualization tool manufactured by GE, StentVizTM.
After the early use of ICL in calcified plaques the first report on the management of stent underexpansion came out as a case report12. It was later followed by the publication of a 13-patient registry from 6 different centers that used OCT-guided ICL to treat stent underexpansion without MACCE at 30-day follow-up.13
These days the European-Canadian CRUNCH registry is being published including 70 patients with stent underexpansion and a rate of device success of 92.3%. The in-stent minimal lumen diameter increased from 149 mm ± 0.73 mm to 2.41 mm ± 0.67 mm (P < .001) while stent expansion went all the way up to 124.93% ± 138.19% (P = .016). No in-hospital complications or MACCE were reported .14
In conclusion, the ESV visualization tool manufactured by GE—StentVizTM—is a new imaging modality to visualize coronary stents.15 This technology consists of a software that improves the image quality of stent struts by acquiring cine cardiac imaging using the markers of a deflated balloon to compensate for cardiac movement. The result is an improved image of the stent that allows detailed assessments of the expansion, architecture, and position of the stent in relation to other stents. StentVizTM is a new ESV platform that uses a non-linear registry process based on balloon and intracoronary guidewire markers to compensate for the non-linear deformity of coronary artery. Theoretically, this feature can generate a more precise representation of the stent compared to algorithms that are based on a linear technique targeted at balloon markers only. Also, the StentVizTM visualization tool is unique because it facilitates guidewire removal.16,17
The ESV algorithm is divided into 4 big aspects that are image acquisition, imaging direction, image combination, and image processing on screen.
With simple tools like the ESV technology plus a rapidly exchangeable balloon catheter that generates intracoronary lithotripsy we can solve very complex cases like the ones described herein even for the lack of intravascular images.
Conclusions
The use of intracoronary lithotripsy (ICL) and enhanced stent visualization (ESV) to guide angioplasty can be an affordable, highly effective tool to treat stent underexpansion in the routine clinical practice.
-
Guedeney P, Claessen BE, Mehran R, et al. Coronary Calcification and Long-Term Outcomes According to Drug-Eluting Stent Generation. JACC Cardiovasc Interv 2020 Jun 22;13(12):1417-28.
-
Stentviz, an Innovative Visualization Tool For Assessing Stent Positioning, Spotlighted By GE Healthcare At TCT, San Francisco, California, USA. September 24, 2009.
-
Bowers TR, Stewart RE, O’Neill WW, et al. Effect of Rotablator atherectomy and adjunctive balloon angioplasty on coronary blood flow. Circulation 1997 Mar 4;95(5):1157-64.
-
Raja Y, Routledge HC, Doshi SN. A noncompliant, high pressure balloon to manage undilatable coronary lesions. Catheter Cardiovasc Interv 2010 Jun 1;75(7):1067-73.
-
Díaz JF, Gómez-Menchero A, Cardenal R, Sánchez-González C, Sanghvi A. Extremely high-pressure dilation with a new noncompliant balloon. Tex Heart Inst J 2012;39(5):635-8.
-
Brinton T, Di Mario C, Meredith I, et al. Performance of the lithotripsy system in treating calcified coronary lesions prior to stenting: results from the Disrupt CAD Study. Paper presented at: Transcatheter Cardiovascular Therapeutics; 2016; Washington, DC.
-
Fujimura T, Matsumura M, Witzenbichler B, et al. Stent Expansion Indexes to Predict Clinical Outcomes: An IVUS Substudy From ADAPT-DES. JACC Cardiovasc Interv 2021 Aug 9;14(15):1639-50.
-
Ali ZA, Nef H, Escaned J, et al. Safety and Effectiveness of Coronary Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Stenoses: The Disrupt CAD II Study. Circ Cardiovasc Interv 2019 Oct;12(10):e008434.
-
Hill JM, Kereiakes DJ, Shlofmitz RA, et al. Intravascular lithotripsy for treatment of severely calcified coronary artery disease: the Disrupt CAD III study. J Am Coll Cardiol 76(2020),2635-2646.
-
Saito S, Yamazaki S, Takahashi A, et al. Intravascular lithotripsy for vessel preparation in severely calcified coronary arteries prior to stent placement: primary outcomes from the Japanese Disrupt CAD IV study. Circ J 2021;85(6):826-33.
-
Peralta S, Fernández Pereira C, Agatiello C, et al. Angioplastia en lesiones coronarias severamente calcificadas. Experiencia inicial con litotricia intravascular coronaria en la Argentina. Serie de casos de intervención percutánea y revisión de la bibliografía. Revista Argentina de Cardioangiología Intervencionista 2021;(02):0088-0092.
-
Morabito G, Tripolino C, Tassone EJ, Grillo P, Missiroli B. A Case of Stent Under-Expansion due to Calcified Plaque Treated with Shockwave Lithoplasty. Cardiology 2018;141(2):75-7.
-
Yeoh J, Cottens D, Cosgrove C, et al. Management of stent underexpansion using intravascular lithotripsy-Defining the utility of a novel device. Catheter Cardiovasc Interv 2021 Jan 1;97(1):22-9.
-
Tovar Forero MN, Sardella G, Salvi N, et al. Coronary lithotripsy for the treatment of underexpanded stents; the international multicentre CRUNCH registry. EuroIntervention 2022 Mar 23:EIJ-D-21-00545.
-
Cordova J, Aleong G, Colmenarez H, et al. Digital enhancement of stent images in primary and secondary percutaneous coronary revascularization. Eurointervention 2009;5(Suppl D):D101–D116.
-
Bismuth V, Vaillant R, Funck F, Guillard N, Najman L. A comprehensive study of stent visualization enhancement in X-ray images by image processing means. Med Image Anal 2011;15:565-76.
-
StentViz Enhanced Stent Visualization. Dr. Morice, Dr. Lefèvre, Dr. Hovasse, Dr. Chevalier, Dr. Louvard Institut Cardiovasculaire Paris Sud, Massy, France. September 07, 2009
Centro CECI. CABA. Argentina.
Centro CECI. CABA. Argentina.
Centro CECI. CABA. Argentina.
Centro CECI. CABA. Argentina.
Centro CECI. CABA. Argentina.
Autor correspondencia
Centro CECI. CABA. Argentina.
Correo electrónico: jmieres@centroceci.com.ar
Para descargar el PDF del artículo
Intracoronary lithotripsy for stent underexpansion resolution: utility of enhanced stent visualization or StentVizâ„¢
![]() Haga click aquí
Haga click aquí
Para descargar el PDF de la revista completa
Revista Argentina de CardioangiologÃa intervencionista, Volumen Año 2022 2
Revista Argentina de CardioangiologÃa intervencionista
Issue # 2 | Volumen
12 | Año 2022

The origins of Interventional Cardi...
Rubén Piraino
CRISPR-Cas9 as protection therapy a...
David Vetcher
The emergence of coronary intravasc...
Sukhdeep Bhogal y cols.
Endovascular resolution of complica...
Macarena Matus de la Parra y cols.
Intracoronary lithotripsy for stent...
Juan Mieres y cols.
Critical limb ischemia: case presen...
Deysi Vanessa Cuadros Morales
Transcatheter aortic valve replacem...
José MarÃa Milanesi y cols.
Venous thoracic outlet syndrome, an...
Jorge Cortez y cols.
Letter from the President of CACI
MartÃn Cisneros
Etiquetas
underexpansion of the stent, IVL, intracoronary lithotripsy, StentVizâ„¢, ESV, enhanced stent visualization
Tags
subexpansión del stent, IVL, litotricia intracoronaria, StentViz™, RVS, realce de la visualización del stent

Intracoronary lithotripsy for stent underexpansion resolution: utility of enhanced stent visualization or StentVizâ„¢
Autores
Juan Mieres, Carlos Fernández-Pererira, Diego Ascarrunz, MatÃas RodrÃguez-Granillo, Alfredo E RodrÃguez
Publicación
Revista Argentina de CardioangiologÃa intervencionista
Editor
Colegio Argentino de Cardioangiólogos Intervencionistas
Fecha de publicación
2022-06-30
Registro de propiedad intelectual
© Colegio Argentino de Cardioangiólogos Intervencionistas






Reciba la revista gratis en su correo

Suscribase gratis a nuestra revista y recibala en su correo antes de su publicacion impresa.